Written and reviewed by the Ultralight Team.
If your patients have started asking about peptides, GLP-1s, continuous glucose monitors, or what their Oura ring is really telling them, you've already brushed up against longevity medicine, whether you've used the term or not.
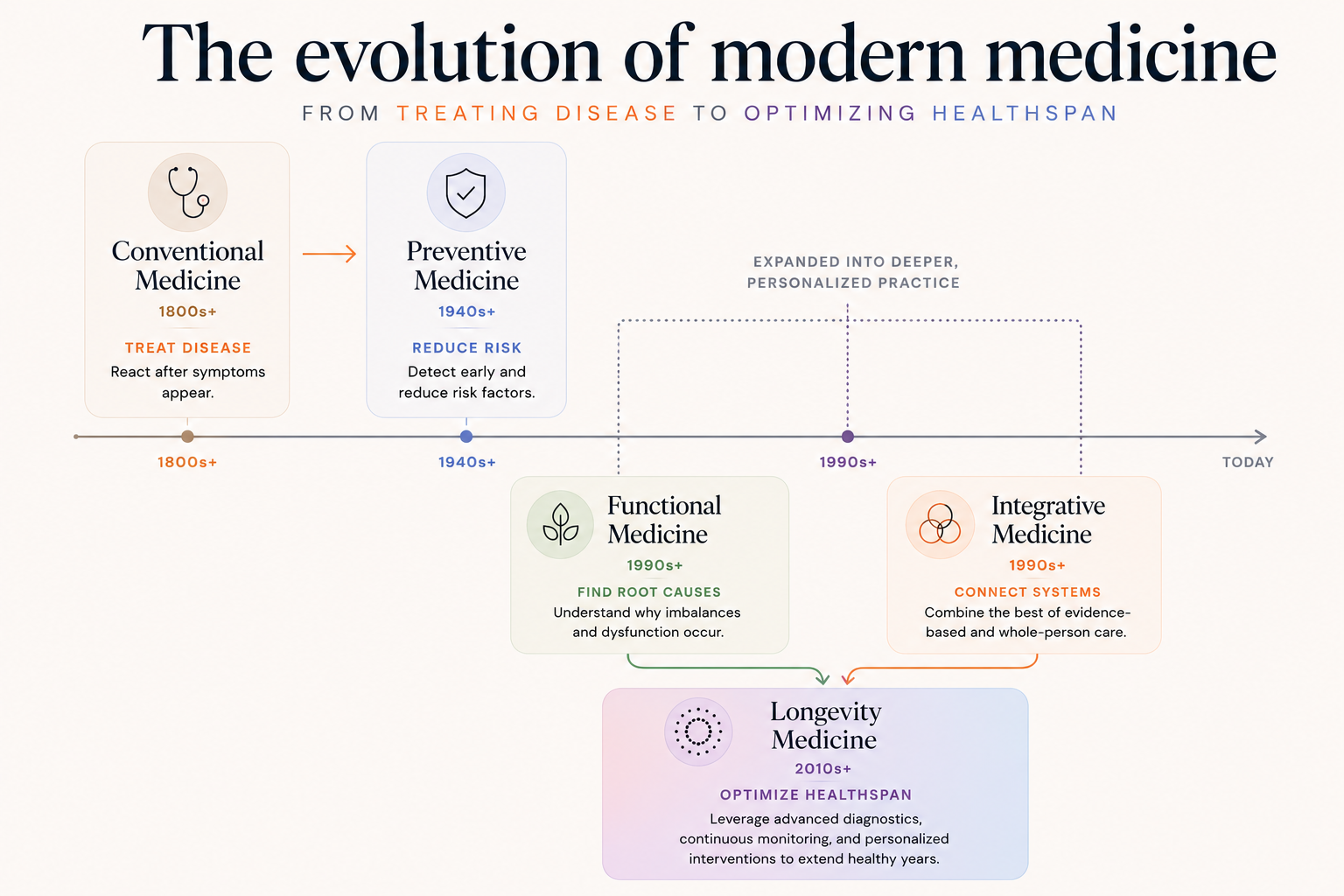
Longevity medicine sits alongside functional and integrative medicine as modern extensions of preventive medicine. All three took preventive medicine's intent and went deeper with advanced diagnostics, continuous monitoring, and personalized protocols. Longevity medicine evolved out of what was originally called anti-aging medicine in the 1990s and 2000s, then rebranded as "longevity medicine" as the field matured.
Demand for longevity care has grown sharply in the past few years thanks to research from David Sinclair, Peter Attia's 2023 bestseller Outlive, Bryan Johnson's quantified "Don't Die" experiment, and institutions like the Buck Institute for Research on Aging. A new generation of cash-pay clinics like Neko Health, Humanaut, and Biograph and physician-led practices like Wild Health and Extension Health have moved the conversation from niche to mainstream.
This guide is for clinicians evaluating longevity medicine as a practice direction. It covers what longevity medicine actually is, how it differs from functional, preventive, and concierge medicine, the diagnostic and protocol stack it requires, the five pillars that define an effective longevity practice, what it takes operationally to deliver it, and the market signals that suggest now is the moment to build.
What is longevity medicine?
Longevity medicine is a proactive, data-driven approach to clinical care that aims to extend both lifespan (how long you live) and healthspan (how well you live). Healthspan is the number of years you live without chronic disease or symptoms, and it’s the metric longevity medicine is optimizing for.
Longevity clinicians use comprehensive baseline testing, continuous monitoring, and personalized intervention to manage how a patient's biology is trending over time. The field is organized around the diseases most likely to cause death: cardiovascular disease, cancer, metabolic dysfunction, and neurological decline. It works backwards from those endpoints, tracking upstream signals like insulin resistance, hormonal decline, and cardiovascular risk factors years before they produce symptoms a conventional clinician would flag.
Longevity medicine is often assumed to be the domain of extreme optimizers (e.g., people tracking every biomarker and spending like Bryan Johnson). That association is not wrong, but it is incomplete. The work those early adopters did helped prove the model and brought tools, data, and awareness into the mainstream that now benefit a much broader patient population.
In practice, longevity medicine applies to anyone who wants to understand their personal disease risk earlier and use that information to change their biology. That includes adults in their 30s and 40s who want to get ahead of risk while their biology is still highly modifiable, men and women navigating the hormonal shifts of midlife, and people with significant family history who want more than "let's watch it." It also applies later than most people expect. The data shows that meaningful improvements to healthspan are achievable even in your 60s and 70s. The unifying trait is a preference for proactive over reactive care.
The Longevity Medicine Stack: diagnostics and protocols
A longevity visit goes significantly deeper than a standard annual physical. Where a standard panel covers 30 to 50 markers once a year, a comprehensive longevity panel covers 350 or more and revisits them on a regular cadence. The stack typically includes:
- Advanced biomarker testing. Cardiovascular markers (ApoB, Lp(a), hs-CRP, advanced lipid panels), metabolic markers (fasting insulin, HOMA-IR, continuous glucose), hormonal panels, inflammatory markers, genetic risk factors, and organ-function panels across multiple systems.
- Advanced imaging. DEXA scans for body composition, lean mass, and bone density. CT calcium scoring and CT angiography for cardiovascular structural risk. Other imaging as indicated by individual risk profile.
- Performance testing. VO2 max for cardiorespiratory fitness and biological age. Grip strength as a longevity proxy. Body composition and functional movement assessments.
- Continuous monitoring. Continuous glucose monitors, wearables, and sleep trackers that capture how a patient's biology responds to real-life inputs, food, exercise, stress, sleep, in real time rather than once a year.
- Hormone and metabolic optimization. Comprehensive hormone testing and, where indicated, medically supervised use of hormone replacement, peptide therapy, GLP-1s, and targeted supplementation. Perimenopause and andropause protocols sit inside this layer.
- Personalized longevity protocols. A unified plan integrating nutrition, training, sleep, supplementation, and prescription interventions, designed around the patient's specific data and updated as the data evolves.
The clinician's job is to integrate all of this into a single coherent picture of where the patient is and where they are headed, and to update the plan as new data arrives.
What it takes to practice longevity medicine
Building an independent longevity practice involves four operational layers beyond the clinical work itself.
Training and credentialing. Most longevity clinicians come from internal medicine, family medicine, or emergency medicine backgrounds and add longevity-specific training through programs like the American Academy of Anti-Aging Medicine (A4M) Fellowship, the Kalish Institute Longevity Certification, or fellowship programs at academic centers like the USC Leonard Davis School of Gerontology. Certification is not legally required, but it shapes credibility and referral patterns.
Diagnostic and lab partnerships. Longevity practice depends on access to specialty labs that accept direct clinician orders (such as Boston Heart Diagnostics, DUTCH Test, and Galleri), imaging centers for DEXA scans and CT calcium scoring, and validated wearables (Oura, Whoop, and Levels CGM) that can feed data into the clinical record. Many of these partnerships are now available without institutional affiliation, which was the bottleneck five years ago.
Patient population and business model. Longevity practice is almost always cash-pay or membership-based. Typical pricing ranges from $3,000 to $10,000 per patient per year, with deeper-stack programs priced higher. The model works because the patient population, often professionals in their 30s through 60s, expects deep care and is willing to pay for it directly. Insurance billing is rare (Parsley Health recently became the first functional and longevity medicine provider to accept insurance nationwide. If Parsley Health’s model scales, similar coverage for longevity services will soon follow.) Some practices also accept HSA and FSA funds for eligible services.
Clinical infrastructure. This is the layer that has changed the most in the past two years. Independent practice used to require a team to handle documentation, lab integration, wearable data ingestion, patient communication, and follow-up tracking. AI-native EHR infrastructure now handles a meaningful portion of that operational load. A 2026 study of more than 8,500 clinicians found that AI scribe use reduced documentation time by 16 minutes per day and EHR usage by 13 minutes per day, with the most pronounced gains for primary care clinicians and heavy users. Multi-modal data synthesis tools bring labs, wearables, and imaging into a single clinical view. Among Ultralight customers, the result is 10 to 15 hours reclaimed per clinician per week, a 25% increase in patient capacity, and 10% higher profit margins.
Why now: market signals
Three signals make this a meaningful moment for clinicians considering longevity medicine.
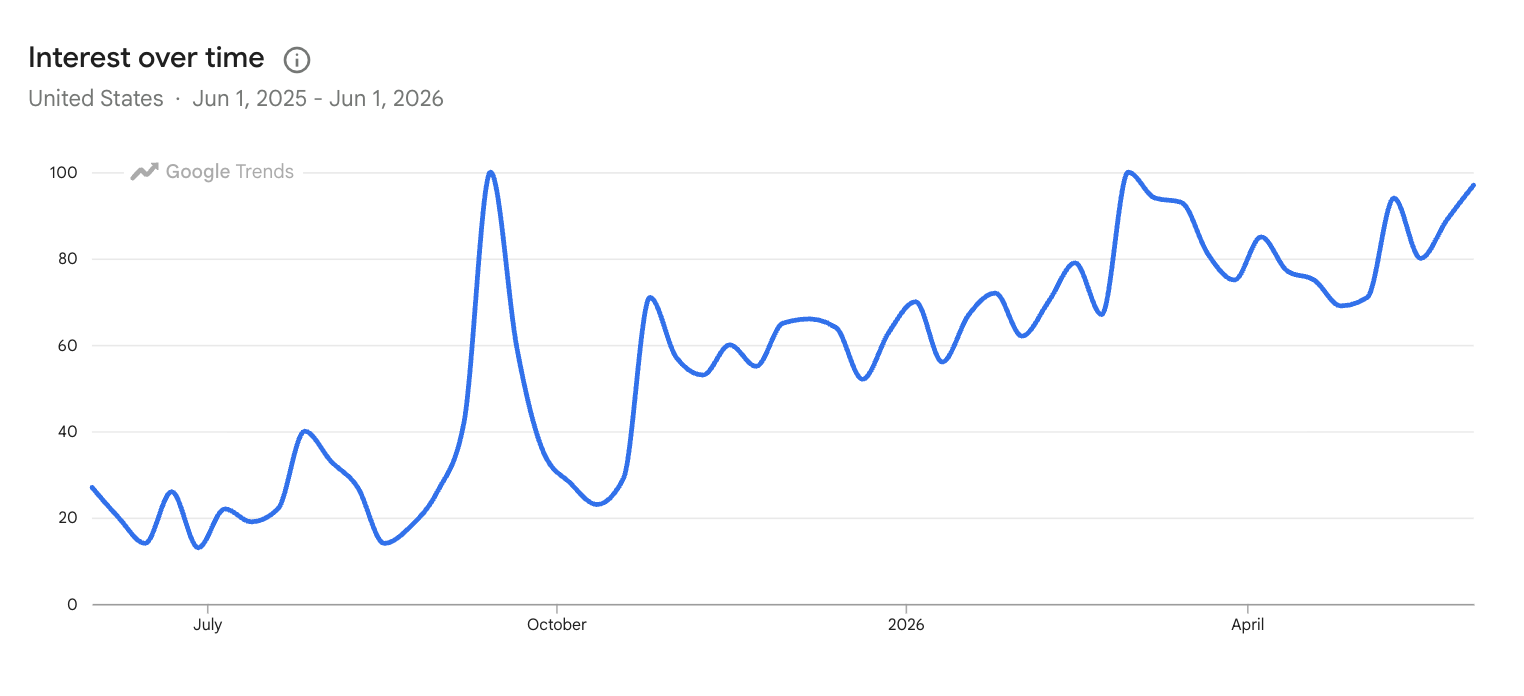
Demand is accelerating fast. Interest in "longevity medicine" has more than tripled in the United States over the past year, according to Google Trends. Adjacent queries (longevity medicine near me, best longevity doctors) show similar growth curves. Peter Attia's Outlive has sold more than 2 million copies since its March 2023 publication and remains a #1 New York Times bestseller. Bryan Johnson's Blueprint raised $60 million in 2026 to scale his "Don't Die" protocol, backed by a Netflix documentary that pushed the topic into mainstream consumer awareness. This is no longer an emerging interest. It is a category in the middle of an inflection.
The patient is arriving with data. Oura's May 2026 IPO filing, at a target valuation above $10 billion with five million paid members, is the clearest signal that wearable biometric data is now mainstream consumer infrastructure. A patient walking into a longevity visit with three years of HRV, sleep, and continuous glucose data expects a clinician who can integrate it. A 15-minute conventional visit has nowhere to put that data. A longevity visit is built for it.
Independent infrastructure is finally viable. Specialty labs accept direct orders. Cash-pay and membership models are normalized. AI-native EHR infrastructure handles the operational load that used to crush small practices. The first wave of longevity-only clinics, Peak Health, Function Health, Fountain Life, has shown the model works. The opportunity now is for individual clinicians to build their own version of it, supported by AI-native platforms like Ultralight that make solo and small-group practice possible.
5 steps to get started with longevity medicine
Want to go deeper into longevity medicine? Here is a practical sequence to get started.
1. Get trained. Start with a structured credentialing program. A4M's fellowship, the Kalish Institute, and the USC Leonard Davis School of Gerontology are the most established paths. Certification is not legally required, but it will shape how patients and referring clinicians perceive you.
2. Run your own panel. Before you order your first patient panel, run a comprehensive longevity panel on yourself. It will make you a better interpreter of data and a more credible clinician. It also tends to be clarifying about which biomarkers actually matter in practice.
3. Build your lab and imaging network. Establish direct ordering relationships with specialty labs like Boston Heart Diagnostics, DUTCH Test, and Galleri. Identify a local imaging center that offers DEXA and CT calcium scoring. These partnerships are now accessible without institutional affiliation.
4. Define your patient model. Decide early whether you are building a membership practice, a per-visit model, or a hybrid. Set your pricing based on the depth of stack you intend to deliver. Most successful longevity practices charge $3,000 to $10,000 per patient per year.
5. Get your infrastructure right before you scale. The operational load of a longevity practice (lab integration, wearable data, documentation, follow-up) is significant. AI-native platforms like Ultralight are built specifically for this model and can reclaim 10 to 15 hours per clinician per week before your panel is full.
Never miss what's next
Our weekly newsletter covers the latest longevity medicine news, independent practice strategy, and the tools reshaping how clinicians work. Join thousands of clinicians staying ahead of where medicine is going at modernclinician.ai.

