Reviewed by Dr. Lexi Gonzales, written by Ultralight CEO Sunita Mohanty, and edited by Clinician Advocate Amy Maxwell
Most clinicians using AI tools describe the same experience. There’s a quiet sense of relief during the visit because AI is taking notes, but then the same pile of work is waiting afterward.
If you practice functional, integrative, or longevity medicine, you know this problem more intimately than most. Your visits are longer because your patients arrive with wearable data, advanced labs, and their own AI notes. A single new patient encounter can generate three times the documentation of a conventional visit and five times the downstream workflow.
This is the honest state of AI in clinical practice right now. Here's what you need to know about what AI actually does in a practice like yours, where the real time savings are, and how to use these tools without compromising the clinical judgment that makes your medicine different.
The hidden problem: Today’s AI was built for conventional medicine
Most AI coverage glosses over the fact that the large language models powering clinical AI tools were trained on conventional medicine. They excel at cardiology, oncology, and internal medicine, but they are considerably less fluent in the territory where functional, integrative, and longevity practitioners actually work.
Ask a mainstream clinical AI tool about senolytics, methylation clocks, peptide protocols, or stool-based biomarkers, and you will often get a shrug or a red flag suggesting clinical caution in areas where the evidence is actually evolving rapidly. These tools were not built for the medicine you practice, and using them without that awareness is how you end up accepting outputs that do not reflect your clinical reasoning or what your patient's data is actually showing.
This is why AI grounded in a knowledge base that reasons like you matters. Generic AI can summarize a visit, but it can't think through a case.
Where AI can assist today (and what is coming next)
AI today is most mature at the work that surrounds the visit, which includes documentation, pre-visit prep, and synthesis across labs, wearables, and diagnostics. The next wave of AI moves past the visit and into action. AI will soon be able to order your labs, follow up with patient messages, and update your care plans. AI-native systems built specifically for clinical workflow are starting to draft these for your review. They are not standard yet, but the field is heading there fast.
The pace of clinical AI is unlike anything healthcare has seen. What clinicians read about as "in development" one quarter often ships the next, which is why "what AI can do" is a moving target worth checking on each year.
AI in 2026 can assist with:
- Real-time visit documentation (AI scribe)
- Pre-visit synthesis pulled from past notes, labs, and wearables
- Visualized trends across labs, diagnostics, and wearables in one view
- Evidence-based clinical insights to inform recommendations
- Personalized care plans built with AI support
- Automated patient reminders and scheduled follow-ups
- Coding and billing suggestions
- Plain-language patient instructions
We predict AI in the next year will assist with:
- Lab orders drafted from visit context, ready for sign-off
- Follow-up messages drafted contextually from the visit, not just scheduled reminders
- Care plan revisions queued automatically between visits
- Longitudinal pattern detection across multi-month protocols
- Personalized between-visit health reports tailored to each patient
- End-to-end automated workflows from visit to follow-up
Not all AI tools are built the same. Some sit on top of your EHR, some are bolted onto your workflow, and some are built from the ground up for clinical practice.
What are the different types of AI clinical tools?
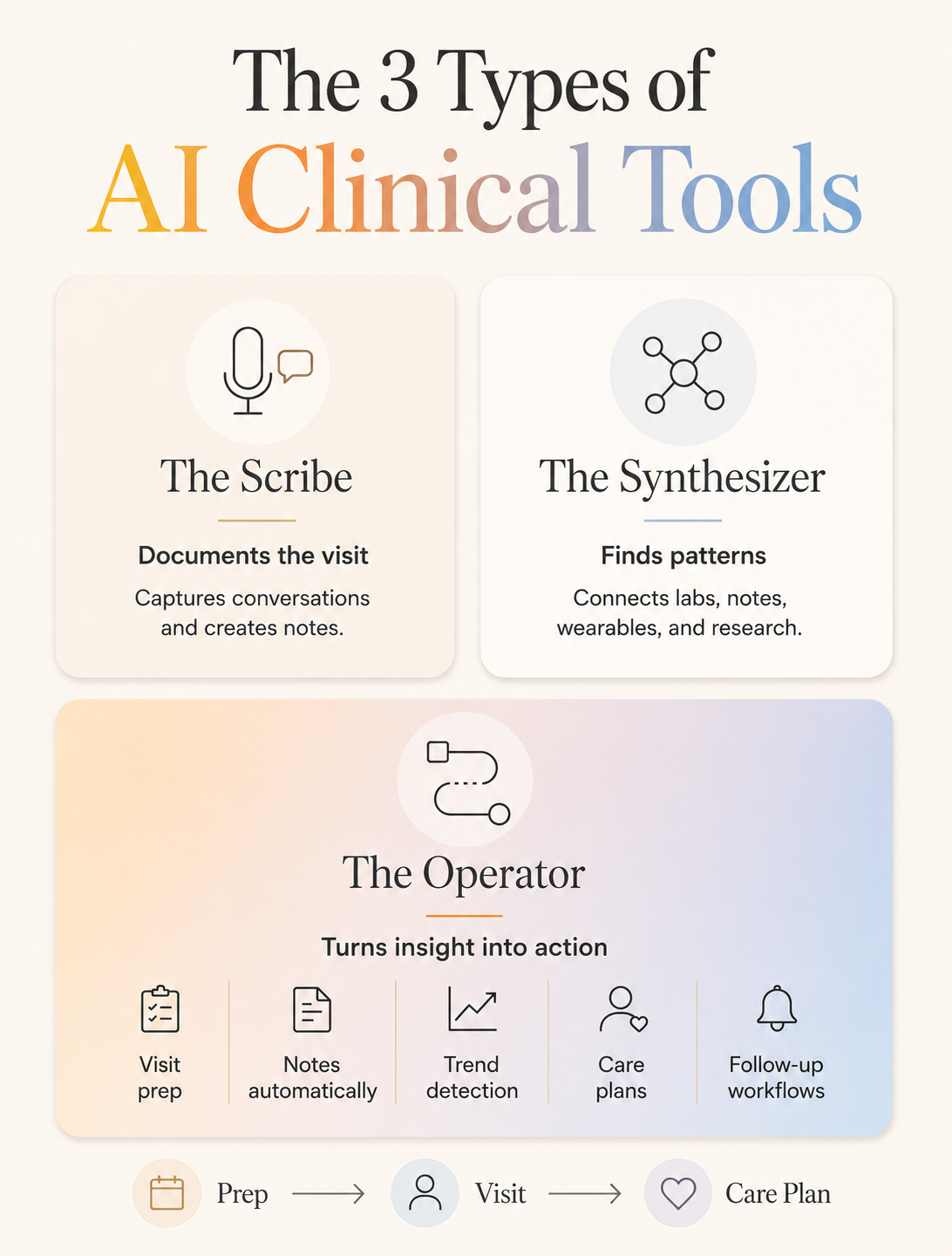
AI tools for functional, integrative, and longevity medicine fall into three layers, each solving a different part of the workflow:
1. The Scribe: Documentation tools like Freed, DeepScribe, Abridge, and Nabla capture visits and generate structured SOAP notes in real time. These were built for conventional medicine, but commonly used by functional, integrative, and longevity practices. This is the highest and fastest return on investment for most clinicians where you can save 2–3 hours per day from documentation alone.
2. The Synthesizer: Tools like OpenEvidence, Elicit, and Consensus search across research sources (e.g., PubMed, clinical trial registries, preprints, guidelines) and synthesize evidence in minutes instead of hours. It’s useful for answering a specific clinical question, pulling citations for a protocol, or pressure-testing your thinking against recent studies. The same conventional-medicine bias noted earlier applies, so expect thinner returns on peptides, senolytics, methylation clocks, and advanced biomarkers.
3. The Operator: An Operator brings the Scribe and the Synthesizer into one platform and adds synthesis across each patient's labs, wearables, and diagnostics. AI-native EHRs like Ultralight document the visit as you talk, surface evidence-based insights, and pull each patient's data into one view so the picture is already drawn before you sit down. They prep visit context from past notes, surface what each patient needs next, support personalized care plans, and automate reminders to keep patients on track between visits. Because the AI is built into the system rather than bolted on, the data flows where it needs to go without you stitching it together.
AI tools built for conventional medicine don't map well to how functional and longevity clinicians actually practice. An AI-native system built specifically for this category operates fundamentally differently than a conventional EHR with an AI feature added on. It organizes the same inputs the way you do with root-cause reasoning first, analyzing multiple systems at once, and protocols that evolve over months and years. Same data, but different reasoning and output.
How to evaluate AI tools for your practice
There are three questions you ask before adopting an AI tool to determine whether it earns a place in your practice or quietly creates more work:
1. What does it do automatically, and what waits for my approval?
AI tools differ in what they handle without per-action input. One tool might queue a reminder for your review while another sends it on a schedule you set once. One might draft a note for review while another saves it directly to the chart. Before adopting any tool, ask the vendor to show you the exact line between "draft and wait" and "execute automatically." That line tells you how much trust you are extending and how much oversight is built in. As tools become more agentic, the question only gets sharper.
2. Does it know my kind of medicine?
This is the biggest gap for functional, integrative, and longevity clinicians evaluating AI tools. If a tool's clinical logic is built on conventional guidelines, it will flag your protocols as outliers. It might mark a lab value as normal that you treat as suboptimal based on functional ranges, or question a supplement protocol that does not appear in its formulary. Ask whether the knowledge base is customizable, whether it learns your protocols, and what happens when your approach diverges from standard.
3. What happens when it is wrong?
Every AI system produces errors. Can you see the reasoning behind each output, or is it a black box? If overriding the AI is harder than doing the task yourself, the tool is not serving you. It is creating a new kind of administrative burden dressed up as efficiency.
Tips for using AI effectively in your medical practice
A 2025 MIT Media Lab study found that people who used AI showed reduced neural engagement and weaker memory formation compared to those who worked on their own. Accepting AI outputs as is won’t work. The solution is to use AI with intention.
Write down your answer before you prompt. Before you open a decision-support tool for a complex case, write down what you already suspect. One sentence is enough. When the AI output arrives you will notice immediately where it confirms your thinking, where it diverges, and where it surfaces something you missed. This keeps your pattern recognition active.
Review the output. Treat every AI output the way you would treat a resident presenting a case. What is the evidence, what is missing, what assumption is baked in. Clinical AI is improving fast but errors still happen, and your review is the safety layer.
Learn how to catch what AI misses. AI output arrives smooth, confident, and internally consistent whether it's right or wrong. The skill of reading AI and noticing what's missing is genuinely new. The more you use AI and check it, the better you will be at recognizing its strengths and weaknesses. You can also protect one task per week from AI entirely to keep your critical thinking skills strong.
The bottom line
The tools aren't perfect yet. The gap between what's marketed as AI-powered and what actually works for functional, integrative, and longevity medicine is real. Knowing that gap exists is part of using these tools well. But the trajectory is clear, and the clinicians who learn how to use AI thoughtfully and intentionally will have a meaningful advantage over those who avoid it or accept it without question
Your training built a capacity for noticing that no language model can replicate. Protect it. And let the tools take care of the rest.
Ready to see what an AI-native operating system looks like in a functional, integrative, and longevity practice? Book a demo with Ultralight.

